The causes of cancer: implications for policy and practice
There are over 200 different types of cancer, and 1 in 2 people in the UK will get cancer in their lifetime (Cancer Research UK). More than 330,000 people are diagnosed with cancer each year in the UK, and over 40% of these cases are linked to a combination of 14 major lifestyle and environmental factors (such as diet and physical activity) that are potentially preventable.
About the research
In its Green Paper Advancing our health: Prevention in the 2020s, the UK government outlined a renewed focus on prevention of ill health. The Integrative Cancer Epidemiology Programme (ICEP) uses cutting edge statistical methods and genetic data (including data on gene products such as proteins, and chemical alterations to genes such as DNA methylation) on 10s to 100s of thousands of people to provide high quality evidence on:
• The causes of cancers
• Factors influencing the progression of cancer
• New ways to predict who will develop or die from these cancers
• New ways to prevent cancer and its progression, including both behavioural and therapeutic interventions.
This knowledge can contribute towards the prevention, early detection and treatment agenda.
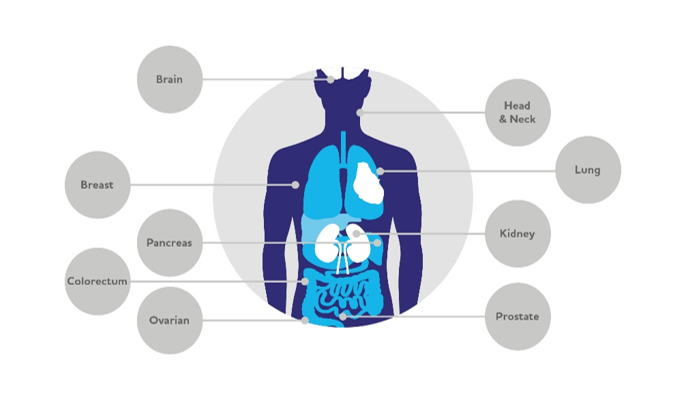
The programme focuses on cancers that are common, present late or have poor survival, including bowel (colorectum), brain (glioma), breast, head and neck, kidney, lung, ovarian, pancreatic and prostate cancer (Figure 1). Understanding the true causes of cancer and why it progresses can enable the development of new ways to prevent cancer and to manage it once Professor Richard Martin, Professor Caroline Relton, Dr Kaitlin Wade, Dr Rebecca Richmond, Dr James Yarmolinsky (University of Bristol) diagnosed. This in turn can help target prevention or treatments to those most at risk - and so have the biggest impact on cancer.
Between 2014 and 2019, ICEP produced over 120 peer reviewed scientific papers and nine database and analytical platforms that are openly accessible and widely used by the scientific and research community around the world. The programme has trained numerous scientists and doctors in population-based cancer sciences, including both at the University of Bristol and at overseas institutions. Several of the programme’s investigators are amongst the most world’s most highly cited researchers. We also have collaborations with the pharmaceutical industry in a programme of work to identify novel drug targets for cancer prevention.
The focus on cutting-edge statistical methods to distinguish cause from association, and the use of largescale human population data and new technologies to provide robust evidence to improve prevention, screening, diagnosis and treatment in cancer are what make ICEP distinct.
This report summarises the research, key findings and policy recommendations.
Key findings and their policy implications
Our large-scale studies highlight multiple areas of intervention to prevent, screen, diagnose and treat cancer.
 Overweight and obesity
Overweight and obesity
Policy Implication
Our updated findings around the importance of overweight and obesity in causing cancer should inform the urgency and content of public health strategies and guidelines for health professionals providing health advice.
 Physical activity
Physical activity
Overall levels of physical activity (e.g. 50 minutes extra moderate activity [such as fast walking] per week or an extra 8 minutes of extra vigorous activity per week) reduce risks of prostate, breast and colorectal cancer by about 50% (Kazmi et al. International Journal of Epidemiology, 2019; Papadimitriou et al. Nature Communications, 2020. See our short video on exercise and cancer.
Policy implication
These findings should inform public health strategies and guidelines for health, education and other professionals providing health advice.
Sleep
Women who report having a “morning preference” have a 40% reduced risk of breast cancer, while women who sleep longer than the recommended seven to eight hours have a 20% increased risk of breast cancer per additional hour slept (Richmond et al. British Medical Journal, 2019). Insomnia too may be a risk factor for other cancers via its influence on smoking habits, as it has been found to increase smoking heaviness and hamper smoking cessation. This points to improving sleep health as a potential additional target when giving smoking cessation advice (Gibson et al. Nicotine & Tobacco Research, 2019).
Policy implication
While further work to investigate the mechanisms underpinning the role of sleep in cancer development is needed, these result support the promotion of healthy sleep by agencies such as the International Agency for Research on Cancer (IARC) as a potential strategy for cancer prevention.
Statins and ovarian and breast cancer
The cholesterol lowering drug - statin - reduces risk of ovarian cancer among both women with no clear family history (sporadic cases) and in women with mutations in BRCA1 or BRCA2 genes who have an elevated lifetime risk of this disease (Yarmolinsky et al. JAMA, 2020).
Policy implication
Though statin drugs cannot currently be advocated as preventive therapy for ovarian cancer these findings support the design of a randomised controlled trial to test whether statin therapy offers a viable approach for cancer prevention (e.g., in women who are BRCA1 or BRCA2 mutation carriers and/or other high-risk groups).
Diagnosing lung cancer
We have found that chemical changes to our DNA, called DNA methylation, are predictive of future lung cancer risk (Battram et al, IJE 2019). A blood test that measures these changes could be used to identify people at high risk of lung cancer. This high-risk group could be targeted for lung cancer screening using CTscans. In 2020, we are conducting studies in additional populations to validate that the biomarker really does improve identification of those with lung cancer and is generalizable across populations.
Policy implication
Research funders should support research aiming to test the utility of these biomarkers in more effectively targeting lung cancer screening programmes. The biomarkers may have additional uses in other high-risk cancer groups beyond lung cancer.
Screening for prostate cancer
Screening for prostate cancer using a one-off PSA test had no effect on prostate cancer-specific or all-cause mortality after an average of 10 years follow-up, in the largest ever randomised trial of prostate cancer screening - the Cluster Randomized Trial of PSA Testing for Prostate Cancer (CAP) (Martin et al. JAMA, 2018). Read more in this evidence summary from CLARHC.
Policy implication
Prostate screening using the PSA test should not be implemented as a preventive tool for prostate cancer. Better tests are needed to identify potentially lethal prostate cancers so that they can be treated early.
 Vitamin D
Vitamin D
Increasing levels of vitamin D does not protect people against developing the eight cancers that we studied. This suggests that, contrary to previous opinion, vitamin D supplementation in the general population would not reduce cancer risk (Dimitrakopoulou et al, BMJ, 2017).
Policy implication
Vitamin D supplements should not be promoted as a protective factor against several cancers.
Funding
This work was supported by grants from a Cancer Research UK Program Grant (C18281/A19169), CRUK Population Research Postdoctoral Fellowships (C52724/A20138, C60153/A28664), CRUK funding for the prostate cancer screening trial (C18281/A24432), the World Cancer Research Fund International (Grant Reference Number: 2015/1421), the Elizabeth Blackwell Institute for Health Research, University of Bristol and the Wellcome Trust Institutional Strategic Support Fund [204813/Z/16/Z], and the National Institute for Health Research (NIHR) Bristol Biomedical Research Centre. RR is a de Pass Vice Chancellor’s Research Fellow at the University of Bristol. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Funding
This work was supported by grants from a Cancer Research UK Program Grant (C18281/A19169), CRUK Population Research Postdoctoral Fellowships (C52724/A20138, C60153/A28664), CRUK funding for the prostate cancer screening trial (C18281/A24432), the World Cancer Research Fund International (Grant Reference Number: 2015/1421), the Elizabeth Blackwell Institute for Health Research, University of Bristol and the Wellcome Trust Institutional Strategic Support Fund [204813/Z/16/Z], and the National Institute for Health Research (NIHR) Bristol Biomedical Research Centre. RR is a de Pass Vice Chancellor’s Research Fellow at the University of Bristol. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
Key publications
Richmond RC et al. Investigating causal relations between sleep traits and risk of breast cancer in women: Mendelian randomisation study. British Medical Journal 2019; 365:l2327.
Mariosa D et al. What can Mendelian randomization tell us about causes of cancer? International Journal of Epidemiology 2019; 816–821: doi:10.1093/ije/ dyz151
Johansson M et al. The influence of obesity-related factors in the etiology of renal cell carcinoma—A Mendelian randomization study. PLoS Medicine 2019; 16(1):e1002724.
Martin RM et al. for the CAP Trial Group. Effect of a Low-Intensity PSA-Based Screening Intervention on Prostate Cancer Mortality: The CAP Randomized Clinical Trial. JAMA 2018;319(9):883–895. doi:10.1001/jama.2018.0154.
Dimitrakopoulou VI et al. Circulating vitamin D concentration and risk of seven cancers: a Mendelian randomization study. British Medical Journal 2017;359:j4761
Yarmolinsky J et al. Association between geneticallyproxied inhibition of HMG-CoA reductase and epithelial ovarian cancer. JAMA.2020: 323(7):1-10. doi: 10.1001/jama.2020.0150
Authors
Professor Richard Martin, Professor Caroline Relton, Dr Kaitlin Wade, Dr Rebecca Richmond, Dr James Yarmolinsky (University of Bristol)
Policy Report 56: June 2020
The causes of cancer: implications for policy and practice (PDF, 3,107kB)
Contact the Researchers
Further information
Find out more about ICEP here.
A full list of the team is available here.
ICEP will continue to build the evidence needed to predict, prevent and treat cancer. We will;
• target common cancers and those that are increasing in incidence
• measure multiple molecular features in a wide range of biological samples
• use state of the art measurements of health behaviours and exposures relevant to cancer risk
• extend the focus on predicting not only cancer occurrence but outcomes (such as recurrence and mortality rates) in patients who are diagnosed with cancer
• ensure that our cancer research findings result in changes to clinical practice or public health policy
• train and mentor a new generation of cancer research leaders in molecular cancer epidemiology